

{kind=link}
Developments in Childbirth in Regency and Victorian England
I have just received a note from James to say that Mary was brought to bed last night, at eleven o'clock, of a fine little boy, and that everything is going on very well. My mother had desired to know nothing of it before it should be all over, and we were clever enough to prevent her having any suspicion of it, though Jenny, who had been left here by her mistress, was sent for home. . . . James went to Ibthorp yesterday to see his mother and child. Letty is with Mary at present, of course exceedingly happy, and in raptures with the child. Mary does not manage matters in such a way as to make me want to lay in myself. She is not tidy enough in her appearance; she has no dressing-gown to sit up in; her curtains are all too thin, and things are not in that comfort and style about her which are necessary to make such a situation an enviable one. Elizabeth was really a pretty object with her nice clean cap put on so tidily and her dress so uniformly white and orderly.
Jane Austen to Cassandra November, 1798
 Jane Austen was a devoted daughter, sister and aunt, but never a wife and mother. Is it possible that her fear of the latter made the former relationship impossible? Many biographers suggest such. To be sure pregnancy during the Regency was a risky business with a nearly 20% mortality rate for the mother. Austen herself lost four sisters-in-law to childbirth. Perhaps that is why she preferred the safety of her writing, calling her books her "own, dear child[ren]." Childbirth in our modern age is no longer a mystery. All of us, male and female, mothers or not, are familiar with the vocabulary of the process at the very least. We have all heard of epidurals, episiotomies, induced labour and dilation as well as horror stories of 24¬-36 hours of labour. All of these facts of modem childbirth were not the reality for mothers in the early 1800s. Indeed, childbirth was the greatest risk to a woman's health and the single most common cause of death. At the beginning of the eighteenth century, all males were excluded from attendance in "lying-in rooms". All decisions were made by female midwives who frequently were not well trained.
Jane Austen was a devoted daughter, sister and aunt, but never a wife and mother. Is it possible that her fear of the latter made the former relationship impossible? Many biographers suggest such. To be sure pregnancy during the Regency was a risky business with a nearly 20% mortality rate for the mother. Austen herself lost four sisters-in-law to childbirth. Perhaps that is why she preferred the safety of her writing, calling her books her "own, dear child[ren]." Childbirth in our modern age is no longer a mystery. All of us, male and female, mothers or not, are familiar with the vocabulary of the process at the very least. We have all heard of epidurals, episiotomies, induced labour and dilation as well as horror stories of 24¬-36 hours of labour. All of these facts of modem childbirth were not the reality for mothers in the early 1800s. Indeed, childbirth was the greatest risk to a woman's health and the single most common cause of death. At the beginning of the eighteenth century, all males were excluded from attendance in "lying-in rooms". All decisions were made by female midwives who frequently were not well trained.
According to reformist Doctor Charles White (1728-1813) a large fire would be built in the room and "by the heat of the chamber, amid the breath of so many people, the whole air is rendered foul, and unfit for respiration." His objections to this practice continue: "As soon as she is delivered, if she is a person in affluent circumstances, she is covered up close in the bed with additional cloaths, the curtains are drawn around the bed, and pinned together, every crevice in the windows and door are stopped closed, not excepting the key hole, the windows are guarded not only with shutters and curtains, but even with blankets, the more effectually to exclude the fresh air, and the good woman is not suffered to put her arm, or even her nose out of bed, for fear of catching cold."
The diet for new mothers was tea and other warm liquors and frequently normal intestinal function would slow because of the lack of solid food and because the new mother remained in bed in a horizontal position for days, sometimes weeks. All these factors increased the risk of developing infection. Medical treatment was harsh by the standards of our time. A famous obstetrician, Dr. Hugh Chamberlain (1630-1700) attended a woman that was "taken ill of a paine in her right side under her short ribb together with a great difficulty of breathing having but 14 weeks to go with child."
Her treatment was "in the space of nine days four vomits, four purges, and caused her to be bled three times to the quantity of eight ounces each time, then gave her something to raise a spitting after which swellings and Ulcers in her mouth followed; about 3 or 4 days after her taking this, she miscarryed, and she continued languishing until she dyed."
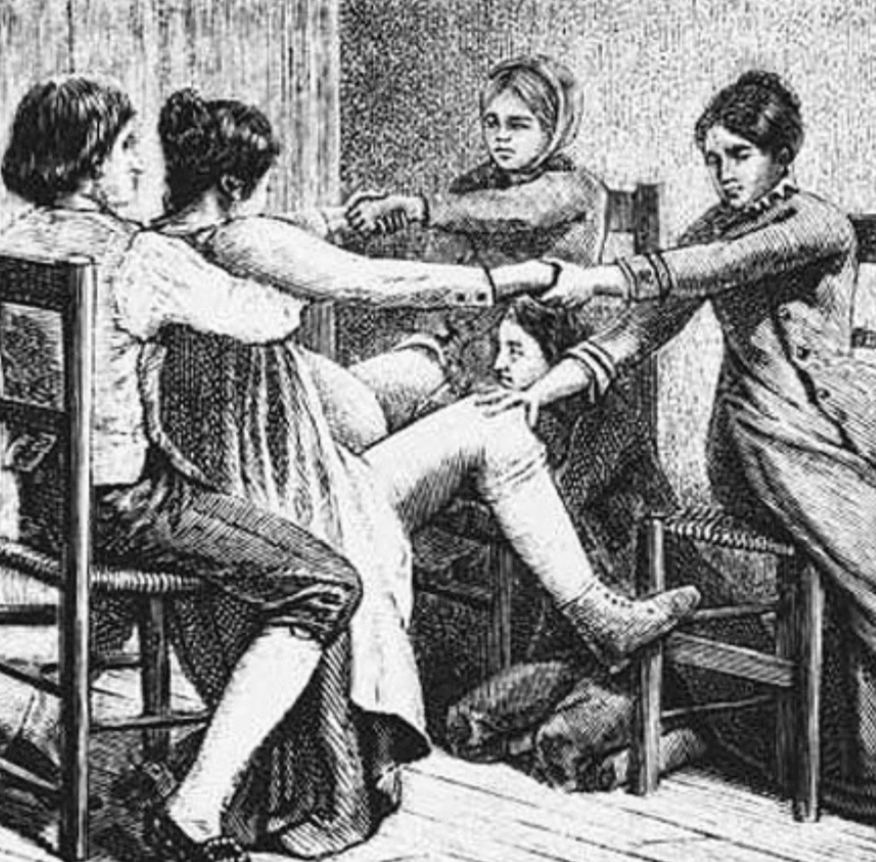
For this treatment, Dr. Chamberlain was found "Guilty of Mal Praxis" and was fined "Ten pounds of lawfull money of England." Not all of the medicine of the time was so appalling. In 1773, an illustrated account of the use of forceps was published. Another book Treatise on the Theory and Practice of Midwifery was first published in 1752 and detailed how "difficult delivery" could be helped. Any "normally skilled" midwife would know the "podalic version" which was to insert her hand into the womb, grasp the feet of the awkwardly placed infant and pull them down out of the uterus. This would require a great deal of physical strength and could be quite potentially harmful to both mother and child. The modern alternative to forced turning is often a caesarean section.
In the 1800s, a caesarean section was always fatal to the mother because of the dirty, unaired and overheated lying-in rooms, lack of anesthetic and antibiotics. This operation was only performed as an attempt to save the child when the mother had died during the labour. If the birth process did not prove fatal, the next greatest risk was a systemic infection that was called puerperal fever, or blood poisoning originating with birth or miscarriage. Often a portion of the placenta or "afterbirth" was retained and gangrene would then claim the life of the new mother.
Doctor Charles White and Doctor Alexander Gordon (1752-99) both supported ideas of better ventilation and clean linen at the lying-in rooms but it was not until the anti-infection work of Dr. Semneelweis, a Hungarian doctor called "The Saviour of Mothers” that mortality rates from childbirth improved. He ordered all students who came from the dissection rooms to bathe their hands in a solution of chlorinated lime before they examined new mothers.
Not surprisingly, mortality rates from childbirth decreased from over eighteen percent to less than six percent. This miraculous idea of hand washing did not come about until the 1840s. Sadly, the death rate of children was appalling in the eighteenth century.
"Two-thirds of the children born in the Metropolitan Area of London in the eighteenth century died before they were five years old and three out of four of these poor little victims failed to reach even their second birthdays."
From Domestic Medicine published in 1784, the death registry indicated that almost one half of the children born in Great Britain died under twelve years of age. As soon as a baby was born in the eighteenth century, it was forcibly fed a "pap". A pap was bread or flour soaked in milk or water. Occasionally, the pap would be pre-chewed by the midwife. A pap was the basis of the diet of the infant until the child was weaned to 'solid' food. You can imagine how difficult this would be to digest! Affluent mothers simply did not breast feed their children and infections were passed to the infants by wet nurses who didn't understand that cleanliness was vital to the new infant's survival. Child mortality made a large family a necessity to beat the odds and have children, especially sons, grow to maturity. Not only was birth a risky proposition but if you had any affection for your spouse, you would be experiencing this blessed event every 18¬24 months, as no effective means of birth control existed. Any methods of birth control, however unreliable, were quite strongly frowned upon by the religious establishment.
Many modern advances that we consider commonplace were an impossibility for women of any class in the 1800s. Anaesthetic, in the form of chloroform or ether, was first used to assist in a difficult delivery on January 19, 1847 by a Scottish physician named James Simpson (1811-1870). Prior to this time, "natural" childbirth was the only option. In addition to the obvious pain of the process, the most common medical treatments of the time included purges and blood-letting as previously mentioned. With the absence of prenatal vitamins and nutrition, most women could be expected to be anaemic during pregnancy. The bleeding of a borderline anaemic mother-to-be was a recipe for disaster. Risks to her health included the possibility of post-partum haemorrhage or a raging infection from the retained placenta or contaminated hands of the midwife or physician. Remember that penicillin was not discovered until the 1920s and was not marketed until 1943! Is it any wonder that childbirth was so very risky?  Even after obstetrical anaesthesia was introduced, it was not universally accepted. The first objection was based on the lack of knowledge of how ether worked. The most common method of administering anaesthesia was to give a dose of chloroform on a cloth that was placed over the patient's nose and mouth. Dr. Simpson gave a large dose that rendered the patient unconscious, in the same fashion as when a patient was to have an amputation or a surgery. The possibility that the infant could be harmed or labour would stop from this use of an anaesthetic agent is a debate that continues today.
Even after obstetrical anaesthesia was introduced, it was not universally accepted. The first objection was based on the lack of knowledge of how ether worked. The most common method of administering anaesthesia was to give a dose of chloroform on a cloth that was placed over the patient's nose and mouth. Dr. Simpson gave a large dose that rendered the patient unconscious, in the same fashion as when a patient was to have an amputation or a surgery. The possibility that the infant could be harmed or labour would stop from this use of an anaesthetic agent is a debate that continues today.
Some practitioners were also concerned about a possible detrimental effect to the woman even after labour as well. Dr. John Snow (1813-1858) used a method of anaesthesia similar to "conscious sedation" of modern times. He would administer the chloroform in a titrated dosage by placing only a few drops on the cloth that the patient then inhaled. This method allowed the patient to be free of pain but to have the ability to follow commands, move her legs and to push when the time came for delivery. Snow attended Queen Victoria's last three deliveries and this method was very successful.
The chief opponent of obstetrical anesthesia was an American physician named Dr. Charles D. Meigs (1792-1869). He shared the view of many physicians of the time that did not feel that obstetrical pain was the same as surgical pain and that anaesthesia posed too great a risk. Some practitioners felt that the pain of labour was mandated by scripture and that anaesthesia was therefore objectionable. Dr. Simpson authored a pamphlet in December 1847, only eleven months after the initial use of anaesthesia in labour to refute this claim. His arguments were so convincing that Queen Victoria was persuaded to attempt anaesthesia with her next delivery and the custom gradually became more widely accepted. How lucky we are to have the choices that we have today! While some of the debates regarding midwives or physicians, home birth or hospital, anaesthesia or natural birth are still continuing, we certainly owe a debt of gratitude to our ancestors. The courage of the women of only two hundred years ago paved the way for the relative comfort and safety we enjoy today. Many other advances in birth practices began during or just after the Regency. The terminology of childbirth changed to increased euphemism: “breeding” became “in the family way” and “lying-in” became “confinement”.
A rise in intervention during childbirth came after tragedy in 1817. Princess Charlotte died 5 hours after 50 hour labor and stillbirth. All Britain mourned and blame fell on Dr. Croft who later committed suicide Opponents of "man-midwifery" advocated the return of female midwives and the Medical establishment responded by advocating quicker use of the newly invented forceps. And finally, in 1828 an English physician suggested the word obstetrician from the Latin "to stand before" to be used to denote a specialist in childbirth instead of the more commonly used names of male midwife, man midwife, madman, accouter, and even androboethogynist. *Lying-in is an old childbirth practice involving a woman resting in bed for a period of time before giving birth. Though the term is now usually defined as "the condition of a woman in the process of giving birth," it previously referred to a period of bed rest required even if there was no medical complications. A 1932 publication refers to lying-in as ranging from 2 weeks to 2 months.

Reprinted by kind permission from Jane Austen's Regency World. The first full colour print magazine about Jane Austen and her era. With additional information from Elena Green's article, Pregnancy and Childbirth for the Histocial Author as well as Romance Reader at Heart and Wikipedia.
Kathleen Charon is a registered nurse and currently lives in Salt Lake City, Utah. She graduated from nursing school in Michigan and works primarily in pediatrics.
Enjoyed this article? If you don't want to miss a beat when it comes to Jane Austen, make sure you are signed up to the Jane Austen newsletter for exclusive updates and discounts from our Online Gift Shop.
Read more
The Subscription Library and the Rise of Popular Fiction
The influence of the "Three Volume Novel" on "Literary Degradation"
Read more
Leave a comment
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.